Chapter 11
Atelectasis
Learning Objectives
- Recognize partial or complete atelectasis of the following on a chest radiograph or computed tomography:
- Right upper lobe
- Right middle lobe
- Right lower lobe
- Right upper and middle lobe
- Right middle and lower lobe
- Left upper lobe
- Left lower lobe
- Recognize complete collapse of the right or left lung on a chest radiograph or computed tomography and list an appropriate differential diagnosis for the etiology of the collapse.
- Recognize lung collapse related to massive pleural effusion on a frontal chest radiograph.
Atelectasis is defined as “diminished volume affecting
all or part of a lung, which may or may not include loss of normal
lucency in the affected part of lung (this finding is not to be
confused with diminished volume produced by resection of pulmonary
tissue)” (1). The term atelectasis is derived from the Greek words ateles and ektasis and means "incomplete expansion" (2,3,4). The term collapse
is used when a whole lobe or lung is involved. Pulmonary atelectasis is
one of the most commonly encountered abnormalities in chest radiology.
Recognizing an abnormality on chest radiography as being caused by
atelectasis can be crucial in understanding the underlying pathology,
such as a case of left upper lobe collapse in an adult with
endobronchial carcinoma obstructing the left upper lobe bronchus. In
this chapter, atelectasis will be used to describe pulmonary loss of volume without substantial filling of alveolar spaces. The term alveolar lung disease
implies filling of alveolar spaces with fluid or other material. This
chapter will review the types of atelectasis based on mechanism, the
signs of atelectasis, and the radiologic manifestations of lobar and
nonlobar atelectasis.
Types of Atelectasis
Pulmonary atelectasis can be divided into six types,
based on mechanism: resorptive, adhesive, compressive, passive,
cicatrization, and gravity-dependent. Whereas atelectasis can be
divided into types based on these different mechanisms, in any given
patient several mechanisms can occur simultaneously.
Resorptive atelectasis, the
most common type, results from resorption of gas from the alveoli when
communications between the alveoli and the trachea are obstructed.
Resorptive atelectasis is therefore also referred to as obstructive atelectasis.
The obstruction can occur at the bronchial or bronchiolar level. The
most important condition producing intrinsic bronchial obstruction is
bronchogenic carcinoma. Other causes of bronchial obstruction include
other primary lung and metastatic neoplasms, inflammatory etiologies
(especially tuberculous or fungal infection), aspirated foreign bodies,
mucous plugging, a malpositioned endotracheal tube (Fig. 11-1),
and extrinsic compression of an airway by neoplasm, lymphadenopathy,
aortic aneurysm, or cardiac enlargement. Resorptive atelectasis is most
commonly caused by obstruction of the small peripheral bronchioles,
from impairment of mucociliary transport and pooling of retained
secretions in the smaller airways. The larger airways are often patent
and filled with air, resulting in air bronchograms within the
atelectatic lung (Fig. 11-2). The presence of
air bronchograms within the atelectatic lung usually, but not always,
indicates the absence of a central obstructing neoplasm. Some of the
conditions known to impair mucociliary clearance include thoracic and
abdominal pain, central nervous system depression, respiratory
depressant medication, general anesthesia, endotracheal intubation, and
inhalation of toxic fumes or smoke (5). Resorptive
atelectasis can also be associated with certain chronic obstructive airway diseases (e.g., asthma, chronic bronchitis, and emphysema), and it can be seen in acute bronchitis, bronchiolitis, and aspiration and other types of pneumonia from obstruction of small airways by inflammatory exudate.
P.196
atelectasis can also be associated with certain chronic obstructive airway diseases (e.g., asthma, chronic bronchitis, and emphysema), and it can be seen in acute bronchitis, bronchiolitis, and aspiration and other types of pneumonia from obstruction of small airways by inflammatory exudate.
 |
FIGURE 11-1. Left lung collapse. Anteroposterior (AP) chest radiograph shows the tip of the endotracheal tube (arrow)
in the right main bronchus, resulting in collapse of the left lung. The
left hemithorax is completely opaque and the mediastinum is shifted to
the left. |
 |
FIGURE 11-2. Bibasilar resorptive atelectasis. AP chest radiograph shows abnormal opacity associated with air bronchograms (arrows) in the lower lobes. There are other areas of linear subsegmental atelectasis more superiorly in the lower lungs. |
Atelectasis resulting from surfactant deficiency is termed adhesive atelectasis.
Insufficient surfactant leads to alveolar collapse; once collapsed, the
alveolar walls tend to adhere, making re-expansion difficult. Diffuse
surfactant deficiency can result from hyaline membrane disease, acute
respiratory distress syndrome, smoke inhalation, cardiac bypass
surgery, uremia, and prolonged shallow breathing (5).
Compressive atelectasis is
caused by any space-occupying lesion of the thorax compressing the lung
and forcing air out of the alveoli. Such space-occupying lesions
include pleural effusion (including empyema), pneumothorax, pleural
tumors, large pulmonary parenchymal masses, large emphysematous bullae,
and lobar emphysema (6). Diaphragmatic hernias and abdominal distension from a variety of causes can also compress the lung.
The distinction between compressive and passive atelectasis
is not clear cut. Any space-occupying mass within the thorax can either
compress the lung or allow the lung to retract, passively, from the
lung's normal elastic recoil mechanism.
Volume loss resulting from decreased pulmonary compliance as the result of pulmonary fibrosis is termed cicatrization atelectasis.
This type of atelectasis is often associated with bronchiectasis in the
affected lung. A number of conditions can result in pulmonary fibrosis
and cicatrization atelectasis - for example, idiopathic pulmonary
fibrosis, sarcoidosis, pneumoconioses, collagen vascular diseases,
chronic tuberculous and fungal infections, and radiation fibrosis.
Normally, the most gravity-dependent portions of lung
receive greater perfusion and have less alveolar expansion than
non–gravity-dependent portions of lung. These gravity-dependent
alterations in alveolar volume are normal but can exacerbate
atelectasis in the dependent portions of the lungs, particularly in
bedridden hospitalized patients with prolonged shallow breathing.
Atelectasis occurring from these forces is termed gravity-dependent atelectasis.
Radiographic Signs of Atelectasis
Radiographic signs of atelectasis are outlined in Table 11-1 (5).
Opacification of atelectatic lung may not be seen until a considerable
loss of volume has occurred. When edema fluid is drawn into the
collapsing lung, pneumonia has resulted in atelectasis, or
postobstructive pneumonitis is present, there can be abnormal
opacification of lung without substantial evidence of volume loss.
Elevation of the diaphragm as a sign of volume loss is most easily
appreciated when comparison is made to a normal baseline radiograph. A
key radiographic feature of upper lobe atelectasis is superior
displacement of the hilus. Conversely, in lower lobe atelectasis, the
hilus is displaced inferiorly. There is usually no hilar displacement
with right middle lobe or lingula atelectasis. Displacement of a
fissure follows the movement of the atelectatic lung and is most
apparent with atelectasis of an entire lobe. Lung surrounding
atelectatic lung often hyperexpands in an attempt to fill in the
missing volume of lung; this is referred to as compensatory
hyperexpansion or sometimes confusingly referred to as compensatory
emphysema. Emphysema is a pathologic condition involving destruction of
alveolar walls. Although emphysematous lungs are invariably
hyperinflated, hyperexpanded lungs are not invariably emphysematous. If
atelectasis affects only one lung, the ribs on that side may come to
lie closer together than the ribs on the contralateral normal side.
This should be distinguished from the approximation of ribs caused by
poor patient positioning at the time the radiograph was obtained.
TABLE 11-1 RADIOGRAPHIC SIGNS OF ATELECTASIS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
One of the pitfalls in diagnosing left lower lobe
atelectasis is artifactual loss of the medial margin of the left
hemidiaphragm and abnormal opacity in the left lower lung as a result
of incorrect angulation of the x-ray beam. Lordotic angulation of the
beam by as little as 10 degrees results in the beam no longer being
tangential to the apex of the hemidiaphragm, creating illusory opacity
in the left retrocardiac region that may be interpreted as atelectasis
or airspace disease in the left lower lobe. Normal appearing diaphragms
and lungs on a lateral view are helpful in making the distinction.
Lobar Atelectasis
In an adult with lobar atelectasis, a central
obstructing neoplasm should always be considered as the underlying
cause. Bronchogenic carcinoma is relatively uncommon in adults under
the age of 40, when bronchial carcinoid tumor is more likely. In
children with lobar collapse, an aspirated foreign body or asthma is
the usual cause. In postoperative patients, the most common cause is a
mucous plug.
With right upper lobe atelectasis, the major and minor fissures move upward (Figs. 11-3, 11-4, 11-5, 11-6);
with severe atelectasis, the lung can approximate the mediastinum and
lung apex. With complete atelectasis, or collapse of the right upper
lobe, the minor fissure parallels the mediastinum and resembles pleural
thickening or mediastinal widening. Compensatory hyperexpansion of the
middle and right lower lobes leads to outward and upward displacement
of the right lower lobe pulmonary
artery. Upward angulation of the right mainstem and lower lobe bronchi may be difficult to appreciate on chest radiography. Two radiologic signs are associated with right upper lobe atelectasis. The Golden S sign, or S sign of Golden (see Fig. 2-11), refers to right upper lobe collapse around a central obstructing mass. The juxtaphrenic peak sign (see Fig. 2-14) refers to a small triangular shadow based on the apex of the dome of the right hemidiaphragm with loss of silhouette of the adjacent hemidiaphragm. On computed tomography (CT), a collapsed right upper lobe appears as a triangular soft tissue density lying against the mediastinum and the anterior chest wall. The border formed by the major fissure posteriorly and the minor fissure laterally is sharp.
P.197
P.198
artery. Upward angulation of the right mainstem and lower lobe bronchi may be difficult to appreciate on chest radiography. Two radiologic signs are associated with right upper lobe atelectasis. The Golden S sign, or S sign of Golden (see Fig. 2-11), refers to right upper lobe collapse around a central obstructing mass. The juxtaphrenic peak sign (see Fig. 2-14) refers to a small triangular shadow based on the apex of the dome of the right hemidiaphragm with loss of silhouette of the adjacent hemidiaphragm. On computed tomography (CT), a collapsed right upper lobe appears as a triangular soft tissue density lying against the mediastinum and the anterior chest wall. The border formed by the major fissure posteriorly and the minor fissure laterally is sharp.
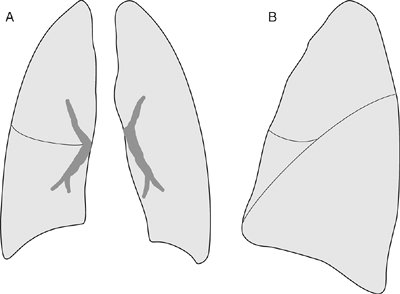 |
FIGURE 11-3. Normal lung volumes and fissures. Frontal (A) and lateral (B)
views of the chest show normal positions of the minor (horizontal,
right-sided) and major (oblique, bilateral) fissures. The major
fissures are often superimposed on the lateral chest radiograph and are
usually not seen on the frontal view. |
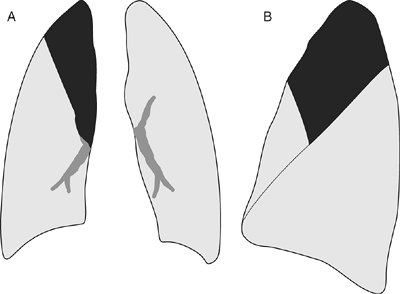 |
FIGURE 11-4. Right upper lobe atelectasis. A: Frontal view of the chest shows elevation of the minor fissure and increased opacification of the right upper medial lung (black area). B:
Lateral view shows elevation of the minor fissure and superior portion
of the right major fissure, as well as opacification of the upper lung. |
 |
FIGURE 11-5. Right upper lobe segmental atelectasis. A:
Posteroanterior (PA) chest radiograph of a 35-year-old man with
lithoptysis (literally "coughing up stones," but representing calcified
lymph nodes that have eroded into the airway, usually secondary to
tuberculosis or histoplasmosis) shows partial collapse of the right
upper lobe. The minor fissure is elevated (arrows), outlining the inferior margin of the opacified, atelectatic lung. Note calcified densities (arrowheads) overlying the opacified lung centrally and peripherally. B: Lateral view shows elevation of the minor fissure (arrows) outlining the inferior margin of the opacified, atelectatic right upper lobe. C: CT shows the smooth and fairly straight fissural margin of the atelectatic right upper lobe (straight arrows), calcified granulomas within the atelectatic right upper lobe (arrowheads), and an obstructing broncholith (curved arrow) within the right upper lobe bronchus (R). |
 |
FIGURE 11-6. Right upper lobe segmental atelectasis. A: PA chest radiograph of a 15-year-old girl with asthma shows elevation of the minor fissure (arrow). B: Lateral view shows elevation of the superior portion of the right major fissure (arrow) outlining a linear band of atelectatic lung. |
Atelectasis of the right middle lobe can be easily
overlooked on the frontal chest radiograph. Loss of silhouette of the
right border of the heart is often seen, but not always. The
atelectatic lobe is more readily recognized on the lateral chest
radiograph as a well-defined linear or triangular band of density lying
between the major and minor fissures (with approximation of these
fissures) and extending downward and forward from the hilum (Fig. 11-7).
The collapsed lobe can be very thin and misinterpreted as a thickened
fissure. On CT scans, right middle lobe collapse appears as a
triangular density bounded posteriorly by the major fissure, medially
by the mediastinum at the level of the right atrium, and anteriorly by
the minor fissure (Figs. 11-8 and 11-9). The posterior boundary should be well defined. Chronic atelectasis of the right middle lobe is referred to as middle lobe syndrome,
a term that was coined in 1948 to describe the presence of right middle
lobe atelectasis and chronic inflammation secondary to enlarged lymph
nodes impinging on the middle lobe bronchus (7).
The middle lobe bronchus is long and narrow, and it is more easily
obstructed at its origin by lymph nodes than are other bronchi. The
syndrome was initially described with tuberculosis, but it may also be
seen in other infections and endobronchial tumors; it may even be seen
in the absence of obstruction.
Combined atelectasis of the right upper and middle lobes
is unusual because there is no single bronchus to the right upper and
middle lobes that does not also supply the right lower lobe. The cause
is almost always cancer beginning in the upper lobe bronchus and
growing down one side of the bronchus intermedius to involve the middle
lobe bronchus. The appearance of combined right upper and middle lobe
atelectasis is similar to that seen with left upper lobe atelectasis.
Combined right lower and middle lobe atelectasis is a
fairly common combination, is seen with obstruction to the bronchus
intermedius, and is similar in appearance to right lower lobe
atelectasis on both posteroanterior (PA) and lateral chest radiographs (Fig. 11-10).
With combined right lower and middle lobe atelectasis, however, the
abnormal parenchymal opacity extends all the way to the lateral
costophrenic angle on the PA view and from the front to the back of the
thorax on the
lateral view. On the frontal radiograph, there is a superficial resemblance to an elevated diaphragm, but the lung above it (right upper lobe) is unusually clear instead of appearing "expiratory." The diagnosis is made much more easily with CT because the bronchi can be identified individually.
P.199
P.200
lateral view. On the frontal radiograph, there is a superficial resemblance to an elevated diaphragm, but the lung above it (right upper lobe) is unusually clear instead of appearing "expiratory." The diagnosis is made much more easily with CT because the bronchi can be identified individually.
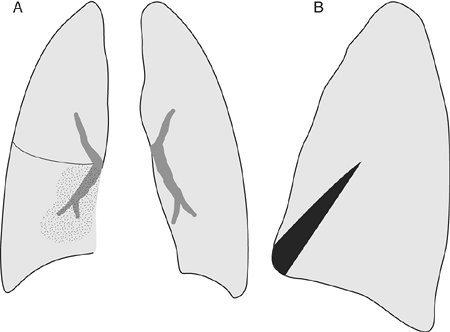 |
FIGURE 11-7. Right middle lobe atelectasis. A:
Frontal view of the chest shows loss of the right heart border and an
ill-defined area of increased opacification in the right medial lung (stippled area). B: Lateral view shows triangular area of opacification (black area) overlying the heart, with approximation of the minor and major fissures. (Reprinted with permission from Collins J. 1996 Joseph E. Whitley, MD, Award. Evaluation of an introductory course in chest radiology. Acad Radiol. 1996;3:994–999. ) |
 |
FIGURE 11-8. Right middle lobe atelectasis. A:
PA chest radiograph of a 52-year-old woman with shortness of breath and
cough shows hazy opacity in the right medial lung and loss of the right
heart border. B: Lateral view shows a linear opacity overlying the heart (arrows), representing the collapsed right middle lobe. C: CT shows a triangular opacity adjacent to the right heart border representing right middle lobe collapse (RML). The right major fissure (solid arrow) is displaced anteriorly compared with the normally positioned left major fissure (dashed arrow). At bronchoscopy, thick secretions were seen in the right middle lobe bronchus. |
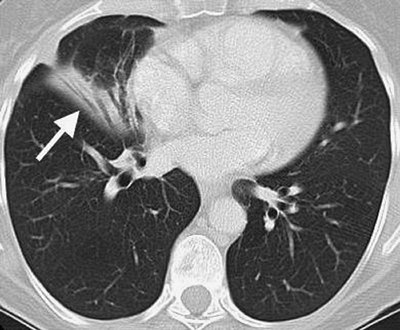 |
FIGURE 11-9. Right middle lobe atelectasis. CT of a 53-year-old man with asthma shows anterior displacement of the major fissure (arrow) and crowding of bronchi in the opacified segment of right middle lobe. |
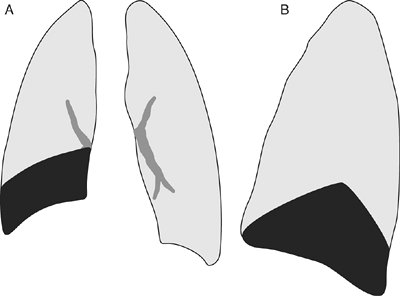 |
FIGURE 11-10. Combined right middle and lower lobe atelectasis. A:
Frontal view of the chest shows elevation of the right hemidiaphragm,
depression of the minor fissure, and increased opacification in the
right lower lung that extends to the lateral costophrenic angle (black area). B:
Lateral view shows depression of the minor and major fissures and
increased opacification of the inferior lung, extending from anterior
to posterior (black area). |
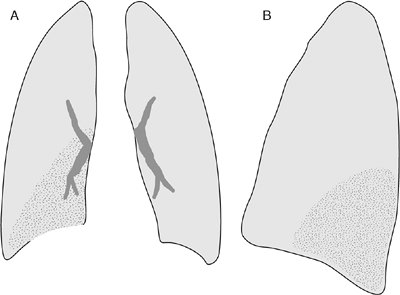 |
FIGURE 11-11. Right lower lobe atelectasis. A:
Frontal view of the chest shows loss of the medial right hemidiaphragm
border, elevation of the right hemidiaphragm, and increased
opacification of the right medial lower lung (stippled area). B: Lateral view shows increased opacification of the posterior inferior lung (stippled area). |
Atelectasis of either lower lobe results in backward and
medial rotation of the major fissure, as well as downward displacement
of the upper half of the fissure. With right lower lobe atelectasis,
the minor fissure can be displaced inferiorly (Figs. 11-11 and 11-12).
The atelectatic lobe lies posteromedially in the lower thoracic cavity,
with a resulting triangular opacity based on the diaphragm and
mediastinum, and with the fissure running obliquely through the thorax (Figs. 11-13 and 11-14).
When a lower lobe collapses completely, it becomes very thin and
appears on the PA chest radiograph as a sliver lying against the
mediastinum. On the lateral radiograph, lower lobe atelectasis results
in loss of the outline of the posterior half of the hemidiaphragm
shadow. Also, with lower lobe atelectasis, the lower vertebrae appear
more opaque than the vertebrae higher up; this results in a situation
that is the opposite of
normal, where the opacity gradually decreases in moving from superior to inferior along the thoracic spine and has been called the spine sign (Fig. 11-15). On CT scans, a collapsed lower lobe produces a triangular opacity in the posterior chest against the spine.
P.201
normal, where the opacity gradually decreases in moving from superior to inferior along the thoracic spine and has been called the spine sign (Fig. 11-15). On CT scans, a collapsed lower lobe produces a triangular opacity in the posterior chest against the spine.
 |
FIGURE 11-12. Bilateral lower lobe atelectasis.
AP supine chest radiograph of a 61-year-old man shows partial loss of
the contours of the hemidiaphragms bilaterally, abnormal opacification
of the lung bases, and inferior displacement of the minor fissure (arrows). |
 |
FIGURE 11-13. Left lower lobe collapse. AP upright chest radiograph of a 17-year-old boy shows downward and medial displacement of the left major fissure (arrows), a triangular area of increased opacification over the left heart, and loss of the left medial diaphragmatic contour. |
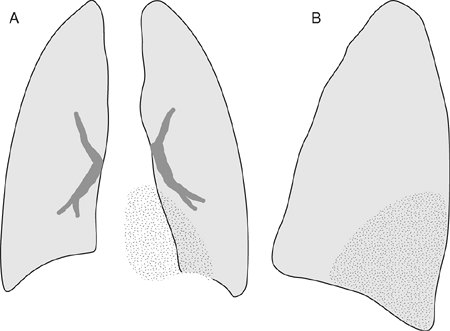 |
FIGURE 11-14. Left lower lobe atelectasis. A:
Frontal view of the chest shows loss of the medial left hemidiaphragm
border, elevation of the left hemidiaphragm, and increased
opacification of the left medial lower lung (stippled area). B: Lateral view shows increased opacification of the posterior inferior lung (stippled area). |
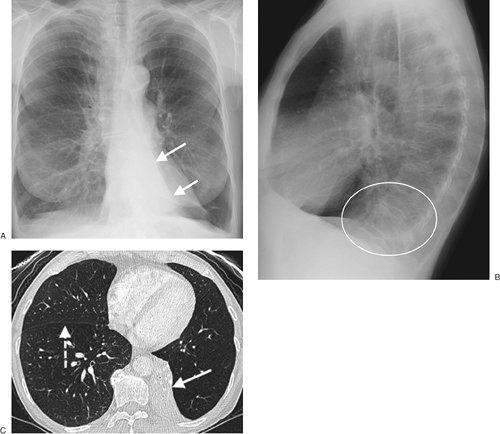 |
FIGURE 11-15. Left lower lobe collapse. A: PA chest radiograph of a 65-year-old woman shows inferior displacement of the left major fissure (arrows) and a triangular area of abnormal opacity projected over the left heart. B: Lateral view shows abnormal opacity overlying the lower spine (circle), the so-called spine sign. C: CT shows the collapsed left lower lobe hugging the spine, outlined laterally by the inferiorly displaced major fissure (solid arrow). Note the normal position of the right major fissure (dashed arrow). |
The radiologic appearance of left upper lobe atelectasis
is markedly different from that of right upper lobe atelectasis because
there is no minor fissure on the left. In left upper lobe atelectasis,
the lobe collapses forward, pulling the expanding lower lobe behind it (Fig. 11-16).
On the frontal radiograph, the atelectatic lobe is seen as hazy
opacification extending out from the left hilum, often reaching the
lung apex, fading laterally and inferiorly (Figs. 11-17 and 11-18).
It is important not to mistake the abnormal parenchymal opacity as
representing pneumonia, and this mistake will not be made if the other
signs of volume loss are appreciated. These signs include loss of the
left cardiomediastinal silhouette, elevation of the left hemidiaphragm,
and shift of the mediastinal structures to the left. With complete
collapse, the upper margin of the aortic arch is visible because the
superior segment of the lower lobe hyperexpands to take the place of
the posterior segment of the upper lobe. This crescentic lucency, which
represents the hyperexpanded superior segment of the left lower lobe
invaginating between the aortic arch and collapsed left upper lobe, is
referred to as the luftsichel sign (see Chapter 2).
This sign can be seen on the frontal chest radiograph and on CT. The
hyperexpansion of the left lower lobe also results in elevation of the
left hilum and outward angulation of the left lower lobe pulmonary
artery. The left main bronchus assumes a near horizontal course and the
lower lobe bronchus runs more vertically than normal. On the lateral
radiograph, the major fissure is displaced anteriorly, paralleling the
anterior chest wall; the atelectatic left upper lobe is seen as an
abnormal band of retrosternal opacification. Left upper lobe
atelectasis in an adult patient is especially important to recognize
because of the frequency with which it is caused by endobronchial
carcinoma.
Complete collapse of either lung results in
opacification of the hemithorax and shift of the mediastinal structures
to the side of collapse (Fig. 11-19). There is
usually hyperexpansion of the opposite lung into the involved
hemithorax. The differential diagnosis of an opaque hemithorax with
volume loss includes congenital absence of a lung (the bony thorax on
the affected side is usually underdeveloped), remote traumatic injury to the bronchus on the affected side (Fig. 11-20), and pneumonectomy (hilar surgical clips provide a clue to the underlying cause of mediastinal shift). Intubated patients are at increased risk of mucous plugging of the airways, and whenever acute lobar or complete lung collapse is seen in this patient population, mucous plugging should be suspected (Fig. 11-21). It is important to recognize lung collapse related to massive pleural effusion, which can (but does not always) result in opacity of the ipsilateral hemithorax and shift of the mediastinum to the opposite side (Fig. 11-22). Parenchymal masses may be obscured on chest radiography when accompanied by lung collapse secondary to central obstruction or massive pleural effusion. In some cases, an opaque hemithorax may represent a combination of a parenchymal mass, lung collapse, and pleural effusion. The overall balance of volume loss and mass effect will determine the position of the mediastinum.
P.202
the affected side is usually underdeveloped), remote traumatic injury to the bronchus on the affected side (Fig. 11-20), and pneumonectomy (hilar surgical clips provide a clue to the underlying cause of mediastinal shift). Intubated patients are at increased risk of mucous plugging of the airways, and whenever acute lobar or complete lung collapse is seen in this patient population, mucous plugging should be suspected (Fig. 11-21). It is important to recognize lung collapse related to massive pleural effusion, which can (but does not always) result in opacity of the ipsilateral hemithorax and shift of the mediastinum to the opposite side (Fig. 11-22). Parenchymal masses may be obscured on chest radiography when accompanied by lung collapse secondary to central obstruction or massive pleural effusion. In some cases, an opaque hemithorax may represent a combination of a parenchymal mass, lung collapse, and pleural effusion. The overall balance of volume loss and mass effect will determine the position of the mediastinum.
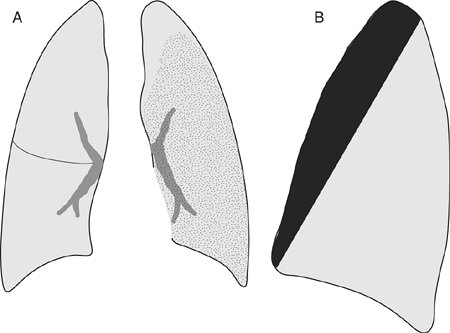 |
FIGURE 11-16. Left upper lobe atelectasis. A:
Frontal view of the chest shows loss of the left heart border,
elevation of the left hemidiaphragm, and increased opacification of the
left lung (stippled area). B: Lateral view shows anterior displacement of the major fissure and increased retrosternal opacification (black area). (Reprinted with permission from Collins J. Joseph E. Whitley, MD, Award. Evaluation of an introductory course in chest radiology. Acad Radiol. 1996;3:994–999. ) |
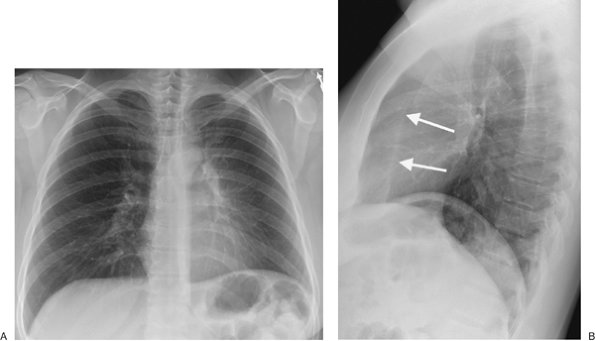 |
FIGURE 11-17. Left upper lobe collapse. A:
PA chest radiograph of a 44-year-old man with a 6-month history of
recurrent pneumonia shows elevation of the left hemidiaphragm, hazy
opacity of the left hemithorax, and loss of the left heart border. B: Lateral view shows anterior displacement of the left major fissure (arrows)
and increased retrosternal opacity. Bronchoscopic biopsy of a left
upper lobe endobronchial mass confirmed the diagnosis of a bronchial
carcinoid tumor as the cause of the left upper lobe collapse. |
P.203
 |
FIGURE 11-18. Left upper lobe collapse. A:
PA chest radiograph of a 54-year-old man with a cavitary left upper
lobe squamous cell bronchogenic carcinoma shows hazy opacification of
the left upper and middle lung, elevation of the left hemidiaphragm,
and loss of a portion of the left upper heart border. Note air–fluid
level within the left upper lobe (arrows). There is a crescentic lucency between the aortic arch and the collapsed left upper lobe (black and white arrowheads) representing hyperexpansion of the superior segment of the left lower lobe (the luftsichel sign). B: Lateral view shows anterior displacement of the major fissure (arrows),
abnormal retrosternal opacification representing the collapsed left
upper lobe, and air–fluid level within the left upper lobe (arrowheads). C: CT shows abrupt cutoff of the left upper lobe bronchus (arrowhead) from an obstructing endobronchial carcinoma and distal collapse of the left upper lobe. Note areas of low attenuation (arrows) within the collapsed left upper lobe, representing trapped mucus, pneumonia, or both. D: CT with lung windowing shows the cavitary cancer in the left upper lobe, with an air–fluid level (arrowheads).
Note hyperexpansion of the superior segment of the left lower lobe
between the aortic arch and collapsed left upper lobe, accounting for
the radiographic luftsichel sign (L). |
Nonlobar Atelectasis
For descriptive purposes, atelectasis can be divided
into several types other than lobar atelectasis, depending on the
anatomic location of the atelectatic lung. Round atelectasis
is a form of chronic atelectasis associated with pleural disease, often
benign asbestos-related pleural disease, and is discussed in Chapter 3.
Discoid atelectasis, also referred to as platelike or linear atelectasis,
is a form of peripheral pulmonary volume loss that is not secondary to
bronchial obstruction. First described in 1936 by Fleischner (8)
and, therefore, also referred to as Fleischner lines, the atelectasis
is disc or plate shaped. Discoid atelectasis usually abuts the pleura
and is perpendicular to the pleural surface; the thickness ranges from
a few millimeters to a centimeter or more, and the lesions are
therefore usually seen as linear or bandlike opacities. The mechanism
of discoid atelectasis is hypoventilation, which leads to alveolar
collapse. Although often of little clinical significance, multiple
areas of discoid atelectasis can be physiologically significant in
certain conditions, such as after general anesthesia.
The radiographic identification of subsegmental atelectasis can be difficult. When atelectasis is present at the subsegmental
level, many secondary pulmonary lobules within the affected segment or lobe may remain aerated, whereas others collapse. In such cases, and when multifocal, the degree of volume loss can be minimal, and the radiograph may show only patchy opacities resembling bronchopneumonia. As more secondary pulmonary lobules collapse within the affected segment or lobe, crowded vessels and bronchi, hilar displacement, or fissural displacement will become apparent.
P.204
P.205
level, many secondary pulmonary lobules within the affected segment or lobe may remain aerated, whereas others collapse. In such cases, and when multifocal, the degree of volume loss can be minimal, and the radiograph may show only patchy opacities resembling bronchopneumonia. As more secondary pulmonary lobules collapse within the affected segment or lobe, crowded vessels and bronchi, hilar displacement, or fissural displacement will become apparent.
 |
FIGURE 11-19. Atelectasis of the right lung.
PA chest radiograph of a 40-year-old man with metastatic frontal sinus
fibrosarcoma shows nearly complete collapse of the right lung, with
only partial aeration of the right upper lobe. The mediastinal
structures are shifted to the right. A large, rounded endobronchial
metastasis is obstructing the right main bronchus (arrowheads), and numerous parenchymal metastases are seen within the left lung (arrows). |
 |
FIGURE 11-20. Collapse of the right lung.
PA chest radiograph of a 30-year-old man with a history of a “punctured
lung” during a motor vehicle crash 11 years previously. There is
complete collapse of the right lung and compensatory hyperexpansion of
the left lung into the right hemithorax (arrows). Note the bronchial cutoff sign on the right (arrowhead), where the bronchus was fractured and healed with granulation tissue. |
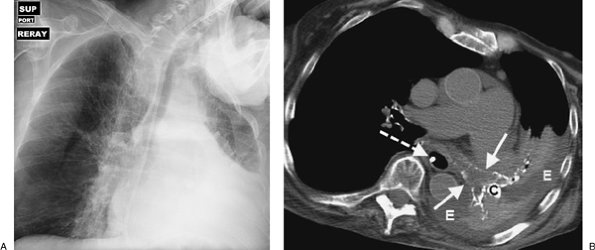 |
FIGURE 11-21. Left lung atelectasis. A:
AP supine chest radiograph of an 82-year-old woman with dementia and
respiratory distress shows nearly complete collapse of the left lung.
Note mediastinal shift to the left. B: CT shows that the left main bronchus (solid arrows),
lingular bronchus, and left lower lobe superior segment bronchus (all
outlined by calcified walls) are airless and filled with
low-attenuation material (mucus). There is a densely calcified left
hilar lymph node (C). Pleural effusion (E) outlines the collapsed left lung. A feeding tube is present within the esophagus (dashed arrow). |
 |
FIGURE 11-22. Massive right pleural effusion.
AP supine chest radiograph of a 55-year-old man with end-stage liver
disease and shortness of breath shows opacification of the right
hemithorax and shift of the mediastinum to the left, away from the
opaque hemithorax. |
Generalized or diffuse atelectasis
is a term used to describe widespread volume loss in the lungs in the
absence of specific signs of linear, segmental, or lobar atelectasis (5).
There can be marked arteriovenous shunting, but the opacification of
the lungs may be mild or unapparent; high positioning of the diaphragm
may be the only radiographic clue to the presence of volume loss. Most
of these cases are interpreted as "poor inspiratory effort." When
generalized atelectasis is associated with diffuse pulmonary
opacification, the interpretation is often diffuse pneumonia or
pulmonary edema. The abnormally high diaphragm provides a clue to the
correct diagnosis, but in practice it is often impossible to
distinguish diffuse atelectasis from poor inspiratory effort or
pulmonary edema.
References
1. Fleischner
Society. Glossary of terms for thoracic radiology: recommendation of
the nomenclature committee of the Fleischner Society. AJR Am J Roentgenol. 1984;143:509–517.
2. Fraser RG, Paré JAP, Paré PD, et al. Diagnosis of Diseases of the Chest. 3rd ed. Philadelphia: WB Saunders; 1988:472–545.
3. Heitzman ER. The Lung: Radiologic Pathologic Correlations. 2nd ed. St. Louis: Mosby; 1984:457–501.
4. Felson B. Chest Roentgenology. Philadelphia: WB Saunders; 1973:92–133.
5. Woodring JH, Reed JC. Types and mechanisms of pulmonary atelectasis. J Thorac Imaging. 1996;11:92–108.
6. Naidich
DP, McCauley DI, Khouri NF, et al. Computed tomography of lobar
collapse. II. Collapse in the absence of endobronchial obstruction. J Comput Assist Tomogr. 1983;7:758–767.
7. Graham EA, Burford TH, Mayer JH. Middle lobe syndrome. Postgrad Med. 1948;4:29–43.
8. Fleischner F. Uber das Wesen der basalen horizontalen Schattenstreifen im Lungenfeld. Wein Arch Intern Med. 1936;28:461.